Article Text

Abstract
Objective To evaluate the effectiveness of two palivizumab programmes targeting high-risk infants, defined by prematurity, diagnosis of comorbidities and geography, and assess potential disparities by neighbourhood income.
Design Controlled, interrupted time series.
Setting Ontario, Canada.
Patients We used linked health and demographic administrative databases to identify all children born in hospitals 1 January 1993 through 31 December 2016. Follow-up ended at the earliest of second birthday or 30 June 2017.
Intervention Palivizumab-eligibility: child was born very preterm and ≤6 months old during respiratory syncytial virus (RSV) season; <24 months old with significant chronic lung or congenital heart disease; or ≤6 months, born preterm or residents of remote regions.
Main outcome Severe RSV-related illness, defined as hospitalisation or death with a diagnosis of bronchiolitis, RSV pneumonia or RSV.
Results 3 million births and 87 000 RSV-related events were identified. Over the study period, rates of severe RSV-related illness declined 65.4% among the highest risk group, eligible infants <6 months (230.6 to 79.8 admissions per 1000 child-years). Relative to changes among ineligible infants <6 months, rates dropped 10.4% (95% CI −18.6% to 39.4%) among eligible infants immediately following introduction of a national palivizumab programme in 1998. Initially, rates were considerably higher among infants from low-income neighbourhoods, but income-specific rates converged over time among eligible infants <6 months; such convergence was not seen among other children.
Conclusions Incidence of severe RSV-related illness declined over the study period. While we cannot attribute causality, the timing and magnitude of these declines suggest impact of palivizumab in reducing RSV burden and diminishing social inequities among palivizumab-eligible infants.
- epidemiology
- health services research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
In the absence of a vaccine, severe respiratory syncytial virus (RSV)-related illness can be prevented through antibody prophylaxis with palivizumab.
Several authors have highlighted that not all children eligible for palivizumab receive treatment or adhere to the monthly dosing schedule necessary for therapeutic effectiveness.
While proven efficacious in clinical trials, research evaluating palivizumab’s real-world effectiveness is lacking through population-based effectiveness studies.
What this study adds?
Rates of severe RSV-related illness substantially declined among high-risk infants since palivizumab was introduced in Ontario in 1998.
Declines in RSV-related admissions among palivizumab-eligible infants were clinically meaningful, but not statistically significant compared with palivizumab-ineligible infants, suggesting reduced effectiveness compared with clinical efficacy.
We observed a convergence of social inequities in RSV-related admissions among palivizumab-eligible children <12 months old, suggesting that publicly funded palivizumab may help reduce social inequities.
Respiratory syncytial virus (RSV) is the most common cause of respiratory tract infection and hospitalisation among children globally, causing over 33 million episodes of illness and 3 million hospitalisations annually.1–3 Approximately 20% of pneumonia and 90% of bronchiolitis cases among children under 6 months of age are attributable to RSV.4–6 RSV infection also has long-term health impacts, such as increased risk of asthma.7 In the current absence of a vaccine, RSV-related illness can be prevented through immunoprophylaxis.8 9 Among children born prematurely without congenital diseases, palivizumab has been found to reduce RSV-related hospitalisations by 80%–85%.10–13 Universal prophylaxis is currently not considered cost-effective given annual costs of administering a complete series typically exceed $6000 ($CAD) per child.14 Consequently, palivizumab is offered only to children at greatest risk of severe RSV-related illness. Most professional organisations, such as the American Academy of Pediatrics and Canadian Pediatric Society, recommend palivizumab for children who are very young during RSV season (eg, <12 months) and born extremely to very preterm or diagnosed with serious lung or heart disease.11 15
There is rich evidence to support palivizumab’s efficacy12 but limited real-world evaluation of effectiveness through population-based studies. Given that receipt requires approval from an administering body and monthly doses are needed throughout the RSV season to maintain therapeutic effectiveness, not all children who qualify receive palivizumab or adhere to the burdensome dosage schedule. Prior studies have shown that characteristics predicting severe RSV-related disease may also predict palivizumab non-adherence.16 17 Travel, culture, inconvenience and lack of understanding of RSV severity are also recognised barriers.8–10 A recent systematic review identified a wide range in palivizumab compliance (25%–100%).18 In a recent Canadian study, adherence with a full palivizumab series was 81% and adherence was greater among younger children, those with siblings and highly educated or non-smoking mothers.17 Critically, even within universal healthcare systems, children from low socioeconomic backgrounds experience reduced access to healthcare services and interventions, such as palivizumab.16 17
Our objective was to conduct a population-based evaluation of the impact of the introduction of two palivizumab programmes on severe RSV-related illness occurring before a child’s second birthday using the comprehensive health administrative and demographic databases available for all children born in Ontario, Canada during 1993–2016. Specifically, we investigated changes following the introduction of Health Canada’s national Special Access Program (SAP) for palivizumab in 1998 and, following licensure in 2002, the Ontario Ministry of Health’s Palivizumab Program for High-risk Infants. We hypothesised that the greatest reductions would be observed within children at greatest risk of severe RSV-related illness, namely palivizumab-eligible infants <6 months-old. We also explored social disparities in palivizumab’s impact by assessing differences across neighbourhood income levels.
Methods
Study population and follow-up
We identified all hospital births occurring in Ontario between 1 January 1993 and 31 December 2016. Health outcomes were identified until the earliest of death, second birthday, moving out of province or 30 June 2017 (end of follow-up).
Data sources
We used several linked population-based administrative health and demographic databases. Births were identified using a provincial birth registry, MOMBABY.19 RSV-related admissions were identified from the Canadian Institute for Health Information’s Discharge Abstract Database (DAD) and deaths from the provincial death registry, Ontario’s Registrar General Death File (ORG-D). Demographic characteristics were determined from MOMBABY, Census, and Immigration, Refugees and Citizenship Canada (IRCC) Permanent Resident databases. These datasets were linked using unique encoded identifiers and analysed at ICES (formerly the Institute for Clinical Evaluative Sciences).
Outcomes
All RSV-related hospitalisations and deaths were identified, representing a composite measure of severe RSV-related illness. RSV-related hospitalisations were those with an RSV-related diagnostic code identified anywhere on the discharge record based on an algorithm recently validated among Ontarian infants by Pisesky et al.20 Specifically, the following International Classification of Diseases 10th and 9th revision (ICD-10 and ICD-9) codes were considered: RSV pneumonia (J12.1, 480.1); acute bronchiolitis (J21.∧, 466.1); or RSV as the cause of disease classified elsewhere (B97.4, 079.6). Similarly, RSV-related deaths were those with the above RSV-related codes identified on the death certificate. Since causes of death are routinely undercoded, to increase sensitivity, we also considered all non-accidental deaths occurring within 30 days of an RSV-related hospitalisation, as done previously.21
Eligibility for federal and provincial palivizumab programmes
Palivizumab eligibility criteria have periodically changed in Ontario; in recent years, a risk scoring tool has been used to assess preterm infants, incorporating factors such as daycare, household crowding and tobacco smoke exposure.22 Such information is not available through administrative data and, currently, there is no identifier for palivizumab receipt. Given challenges in accurately identifying these characteristics and to maximise transferability to other settings with stricter eligibility criteria, we created a three-level variable for children clearly eligible, possibly eligible and clearly ineligible for palivizumab based on standard criteria consistently applied throughout the study period.22–24
Clearly eligible children were: (1) born ≤32 weeks gestational age (wGA) and aged ≤6 months during RSV season (ie, mid-November through March); (2)<24 months with bronchopulmonary dysplasia; (3)<24 months with hemodynamically significant congenital heart disease or (4) born 33–36 wGA, aged ≤6 months during RSV season and living in isolated communities where hospital care is not readily accessible. Possibly eligible children were aged <24 months and previously diagnosed with other congenital heart disease, congenital airway anomalies, or Trisomy 21, and all other preterm (33–36 wGA) infants ≤6 months during RSV season. Additional details are provided in online supplementary appendices A–C.
Supplemental material
Covariates
Given the absence of gestational age data in ICD-9, gestational age groups were determined for all births using a validated algorithm.25 26 Major congenital anomalies were identified from any hospitalisation occurring before the second birthday with ICD-9/10 codes of 740–59 or Q00-99.27 Presence of hemodynamically significant congenital heart disease was determined on the basis diagnostic and procedural codes occurring before the second birthday.28 Rurality was operationalised using the Rurality Index of Ontario (RIO), a continuous measure created for policy purposes.29 Geographic isolation was defined as RIO≥75, following funding incentives for isolated communities.29 Neighbourhood-level income quintile was measured at the dissemination area, Canada’s smallest census area consisting of 400–700 persons. Due to small cell sizes, income was dichotomised in analysis: quintiles 5 and 4 as high-income and quintiles 1 and 2 as low-income.
Statistical analyses
We modelled annual rates of severe RSV-related illness using Poisson regression, including an offset term for log person-time to calculate rates. Years were defined as 1 July through 30 June to capture unique RSV seasons. An interrupted time series design was conducted using a segmented regression approach to assess both step and slope changes following the introduction of each programme: the national SAP in 1998 and the provincial high-risk program in 2002.30
In the secondary analysis of socioeconomic differences by income, we stratified models according to palivizumab eligibility. Given statistical power limitations, we only considered step and slope changes over the entire study period and not by programme.
All analyses were stratified by age at infection:<6, 6–11 and 12–23 months. Analyses were performed in SAS V.9.4 (SAS Institute, Cary, North Carolina, USA).
Results
The study included over 3 million births, with 86 772 RSV-related hospitalisations, accounting for 238 026 bed-days and 58 RSV-related deaths observed among 77 323 children. Bronchiolitis was the most common diagnosis identified among children with severe RSV-related illness (95.2%); 4.6% had a diagnosis of RSV pneumonia and 2.1% had an RSV confirmation recorded on their discharge record. In all, 1.1% of included children were considered clearly palivizumab-eligible and another 4.8% possibly eligible (table 1). Only 4.6% of children with severe RSV-related illness met any of the considered palivizumab eligibility criteria (online supplementary table 1).
Characteristics of children included in the study, that is, all births in Ontario occurring 1 January 1993 to 31 December 2016, stratified by palivizumab eligibility group
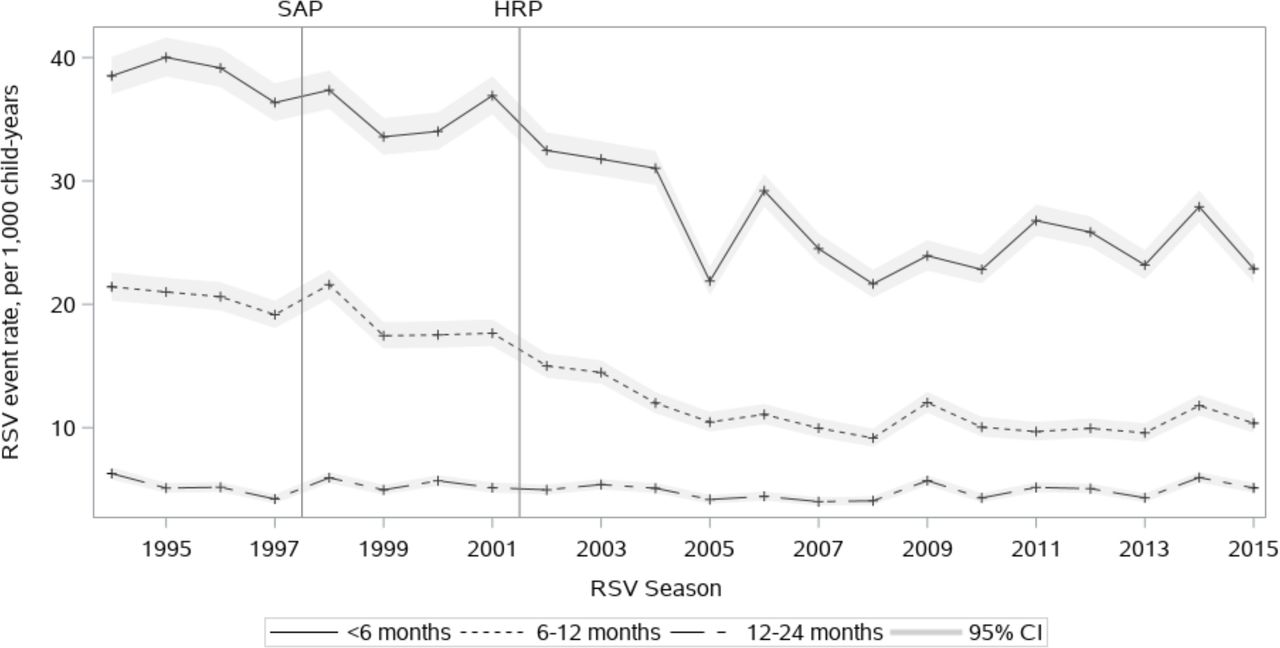
Rates of severe RSV-related illness were substantially higher among infants<6 months, particularly eligible infants (figures 1 and 2). Over the study period, there was a statistically significant trend towards declining rates of severe RSV-related illness among all age groups; rates of decline significantly differed by age (figure 1).

Annual rates (95% CI) of severe RSV-related illness* among all children born in Ontario, 1 January 1993 to 31 December 2016, stratified by age at infection. Average annual change (95% CI) was −2.6% (−2.8 to –2.5), −4.5% (−4.7 to −4.8) and −0.3(−0.6 to −0.1) for<6, 6–11 and 12–23 month-olds, respectively. *Annual rates of RSV-related hospitalisation or death for 1 July through 30 June inclusive. HRP, Provincial High-Risk Palivizumab Program (2002); RSV, respiratory syncytial virus; SAP, National Special Access Palivizumab Program (1998).

Annual observed and predicted rates (95% CI) of severe RSV-related illness* among infants under 6 months of age†, according to eligibility for Ontario’s palivizumab programme; 1993–2016. *Annual rates of RSV-related hospitalisation or death for 1 July through 30 June inclusive. †<6 months of age at the time of admission/death. Model parameter estimates, along with associated 95% CIs and p values, are provided in online supplementary table 2. HRP, Provincial High-Risk Palivizumab Program (2002); RSV, respiratory syncytial virus; SAP, National Special Access Palivizumab Program (1998).
Among palivizumab-eligible infants <6 months, the absolute decline in rates was 65.4% (51.4% to 75.4%) over the study period; in contrast, declines of 41.1% (28.4% to 51.5%) and 31.1% (26.0% to 36.0%) were observed among possibly eligible and ineligible infants<6 months. Among eligible infants <6 months, absolute declines of 18.3% (−9.9% to 46.6%) and 6.7% (−16.6% to 29.9%) occurred the year following the national and provincial programmes (figure 2). Relative to changes among ineligible infants <6 months old, rates dropped an additional 10.4% (−18.6% to 39.4%) among eligible infants (<6 months) immediately following palivizumab’s introduction in 1998; that is, the ‘level change’ among palivizumab-eligible children was −18.3% (−46.6 to 9.9) while the ‘level change’ among palivizumab-ineligible children was −7.9% (−14.7 to 1.2), resulting in a relative ‘level change’ of −10.4 (−39.4 to 18.6) among palivizumab-eligible infants, compared with palivizumab-ineligible infants (online supplementary table 2). Relative to changes within ineligible infants, the improvement in RSV rates observed after the first introduction of palivizumab among palivizumab-eligible infants was not statistically significant.
Within the 6–11-month-old age group, rates of severe RSV-related illness dropped an additional 23.1% (−18.6% to 64.8%) for eligible infants relative to ineligible infants immediately following palivizumab’s first introduction in 1998 (online supplementary figure 1 and table 2); however, RSV rates increased 39.9% (5.7% to 74.1%) relative to palivizumab-ineligible infants following palivizumab’s licensure in 2002. A similar pattern was observed among children aged 12–23 months (online supplementary figure 2 and table 2). See online supplementary table 2 for full model results.
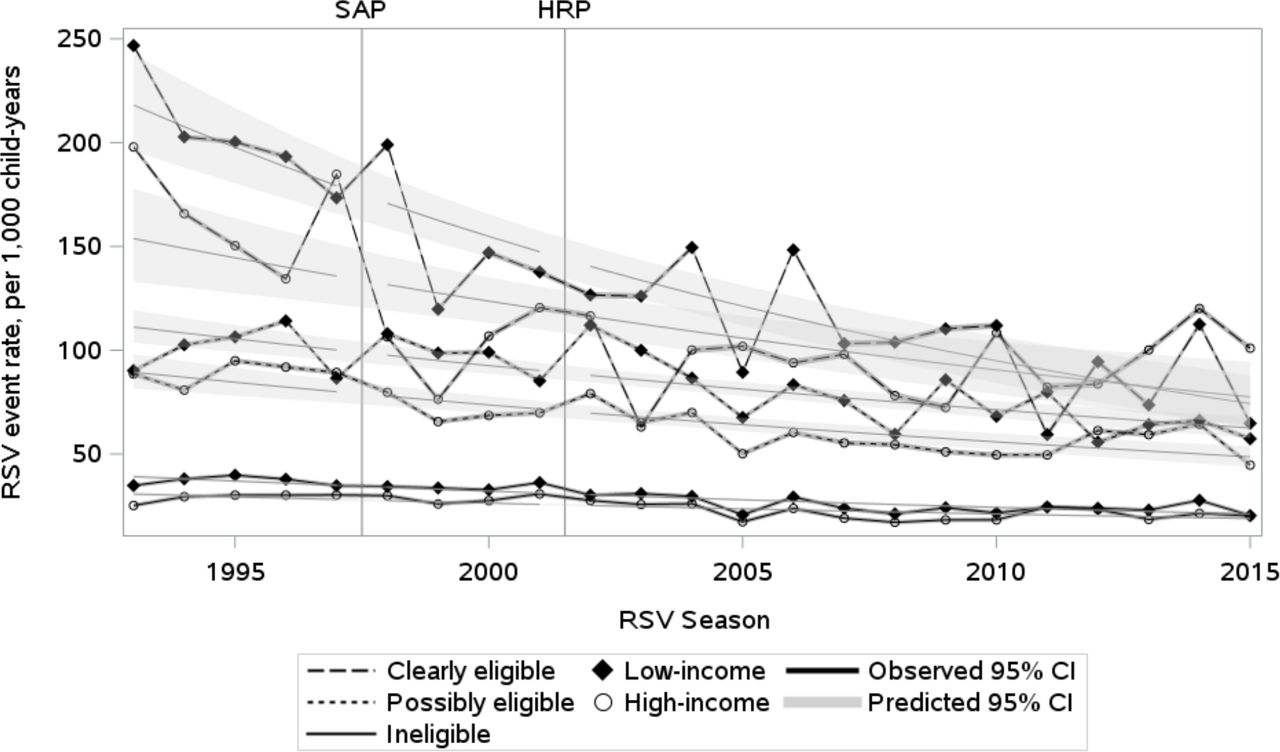
Among infants <6 months, rates of severe RSV-related illness were substantially greater among those from low-income neighbourhoods (figure 3). For example, during the first study year (1993), rates of severe RSV-related illness were 19.8% greater among eligible infants <6 months from low-income neighbourhoods, compared with their high-income counterparts (246.7 vs 197.9 admissions per 1000 child-years). However, among eligible infants <6 months, this income difference narrowed by 1.8% per year on average (p=0.0423), with rates converging during the final 4 years of the study. Specifically, RSV rates declined 4.9% per year on average (p<0.0001) among clearly eligible, low-income infants <6 months; compared with 3.1% among high-income infants (p<0.0001). This gap widened, but not significantly so, among possibly eligible infants <6 months. Among palivizumab-ineligible infants <6 months, this income gap significantly diminished but did not converge. Similar patterns were observed among 6–11-month-olds, though no changes were statistically significant and inequities were less apparent (online supplementary figure 3). No clear income disparities were apparent among 12–23-month-olds (online supplementary figure 4). Full model results are presented in online supplementary table 3.

{kind=link}
{kind=link}
{kind=link}
Annual observed and predicted rates (95% CI) of severe RSV-related illness* among high-income vs low-income infants under 6 months of age**, stratified by palivizumab eligibility. *Annual rates of RSV-related hospitalisation or death for 1 July through 30 June inclusive. **<6 months of age at the time of hospitalisation/death. Annual rate of change between high-income and low-income groups: −1.78 (p=0.0423), 0.16 (p=0.7500) and −0.60 (p=0.0009), respectively, for clearly eligible, possibly eligible and ineligible groups. Model parameter estimates, along with associated 95% CIs and p values, are provided in online supplementary table 3. HRP, Provincial High-Risk Palivizumab Program (2002); RSV, respiratory syncytial virus; SAP, National Special Access Palivizumab Program (1998).
Discussion
In this large, population-based study, rates of severe RSV-related illness declined substantially over the 24-year study period. The greatest improvements were observed among palivizumab-eligible infants <6 months; however, these changes were not statistically significant relative to changes within ineligible infants. Further, we observed that rates of severe RSV-related illness were initially greater among infants<12 months from low-income neighbourhoods, regardless of eligibility, but these disparities diminished among eligible infants over time. While we cannot definitively attribute these effects to the availability of palivizumab, the timing is suggestive of its impact. These observations are consistent with palivizumab efficacy demonstrated in trials and suggest that this efficacy does translate into substantial real-world effectiveness,31 although to a lesser degree.
There is rich evidence supporting palivizumab’s efficacy in various clinical subgroups;9 32 however, there has been scant research into real-world effectiveness. To our knowledge, this is the first population-based evaluation of any palivizumab programme, so there are no comparative studies. However, two US population-based studies have reported on RSV-related admissions over the past two decades and a third on bronchiolitis admissions;33–35 none explicitly evaluated changes due to palivizumab. A 55% decline in RSV-related hospitalisations was observed over 1998–2011 among Californian infants <12 months with high-risk medical conditions (7.6–3.4 per 1000 children), compared with 43% among those without any high-risk conditions.33 Similarly, a 12% decline in RSV-related admissions was observed among US infants <2 years old over 1998–2012; declines of 38% and 10%, respectively, occurred among children with and without high-risk conditions.34 Further, a 17% decline in bronchiolitis-related admissions was reported over 2000–2009 among US children <2 years old.35
Considering the multitude of steps required to receive a full series of palivizumab (eg, parental/provider knowledge of eligibility, administering approval and adherence), effectiveness studies are critical for determining real-world impact. Even within clearly eligible, high-risk infants, real-world effectiveness of these palivizumab programmes was not comparable to trial-based efficacy estimates.3 10 The relative decline in severe RSV among eligible infants <6 months was 65.4% over our study period, with the greatest impact seen immediately following palivizumab’s first introduction in 1998. In contrast, RSV rates declined 41.1% and 31.1%, respectively, over the study period among possibly eligible and ineligible infants <6 months. Improvements were less apparent among older children, for which fewer RSV events occur and palivizumab eligibility criteria are more restrictive.
Ontario’s criteria are considerably comprehensive; most jurisdictions limit palivizumab to young infants born very preterm and with severe heart or lung disease (online supplementary appendix D).24 36 Thus, additional research is required to ascertain the effectiveness of palivizumab programmes in other settings. While we observed clinically meaningful declines in severe RSV among palivizumab-eligible infants, we also observed declines among palivizumab-ineligible infants and the difference between these two groups was not statistically significant. Declines in severe RSV among palivizumab-ineligible children could reflect changes in RSV dynamics, prevalence of cofactors influencing severity of infection (eg, parental smoking) or other factors.16 Both population-based studies of US infants found substantial reductions in RSV-related admissions among low-risk infants, further suggesting improvements beyond palivizumab.33 34
An additional key finding was that the initial gap in RSV-related illness among eligible infants <6 months from high-income vs low-income neighbourhoods entirely diminished over time. While we are unable to attribute this finding definitively to equitable access to palivizumab, the timing is consistent with such an underlying mechanism. This finding is encouraging given that the introduction of novel interventions frequently accentuates health disparities via preferential uptake by the most advantaged.37 38 While multiple studies have shown that children from lower socio-economic backgrounds have increased RSV-related hospitalisation rates, none to our knowledge have explicitly investigated changes in these inequities.16 33 37
While the strengths of this study are related to its population-based nature, these data have limitations. We were unable to determine palivizumab receipt or comprehensively identify all eligibility criteria. However, the distribution of children meeting eligibility criteria in our study was comparable to the Canadian Registry of Synagis (CARESS) (online supplementary table 4).39 Further, in 2015/2016, 3119 children received palivizumab in Ontario;40 nearly 2000 children would have been clearly palivizumab-eligible in our study. Moreover, even though we included all severe RSV-related illness among all children born in Canada’s largest province over multiple decades, we may lack power to detect true differences within eligible groups, particularly older children for which RSV events were rare and few are palivizumab-eligible. We were also unable to ascertain laboratory confirmation of RSV. Given viral tests are inconsistently performed as there are no provincial testing guidelines for RSV, limiting the outcome to laboratory-confirmed RSV would have underestimated the true burden of RSV and biased our results. Similarly, biases in admission practices should be considered; for example, clinicians may be more prone to admit younger children or children with underlying complexities compared with older or less fragile children with a similar level of respiratory distress. In addition to age-stratifying our results, we attempted to further investigate some of these differences, for example, by investigating supplemental oxygen and ventilation use. Unfortunately, diagnostic and procedure codes for these diagnoses/interventions were not consistently available or applied throughout the ICD-9 and ICD-10 eras, limiting our ability to accurately investigate these outcomes over the entire study period and, particularly, during the prepalivizumab (ie, ICD-9) era. These coding considerations also limit ability to look at other changes in practice which may explain part of the decline in RSV-related admissions over the study period; for example, children who were sent home with oxygen therapy to prevent an admission. Moreover, some bronchiolitis admissions would have been due to other pathogens, for example, influenza; however, approximately 85% of bronchiolitis in children are attributable to RSV.1 2 6 20
The major strengths of this study include the ability to study trends at a population-level over a 24-year period. We also incorporated control groups (ie, palivizumab ineligible and possibly eligible children) to account for secular trends not directly influenced by palivizumab, such as changes in medical coding, practice, admissions and cofactors. Controlled interrupted time series analysis with preintervention and postintervention periods are considered the most rigorous quasiexperimental design.30 Nevertheless, these estimates are likely conservative given data limitations.
Conclusion
This large, population-based study spanning multiple decades found that severe RSV-related illness substantially declined among high-risk infants in Ontario, Canada. While we cannot firmly attribute causality, the magnitude and timing of changes, along with diminished social inequities, among palivizumab-eligible infants are noteworthy. While there is rich evidence to support the clinical efficacy of palivizumab, this work provides much needed insights into the real-world effectiveness of palivizumab programmes, which appear to have reduced effectiveness compared with clinical trial estimates. Additional research is required to determine whether, and to what degree, the effectiveness of palivizumab programmes could be enhanced through ensuring therapeutic levels are maintained throughout RSV season (ie, adhering to the monthly dosing schedule) and efforts to promote the availability and uptake of palivizumab among eligible children, particularly where publicly funded.
References
Footnotes
Contributors TF conceptualised the study, analysed the data, interpreted the findings and drafted the manuscript. JDM contributed critically to study design, methods, interpretation and the final manuscript. TAS provided statistical guidance, assisted with statistical interpretation of the results and critically contributed to the final manuscript. ASW created the dataset for analysis and critically contributed to the final manuscript. JCK and DF contributed critically to study design, interpretation and the final manuscript. AG supervised the study design, provided clinical context for study methods and findings and critically contributed to the final manuscript. All authors approve the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding This project was supported by Dr Guttmann’s Canadian Institutes of Health Research (CIHR) Chair in Reproductive, Child and Youth Health Services and Policy Research (Funding Reference Number: APR 126377). Doctoral training support for TF was generously provided by The Canadian Immunization Research Network (CIRN) and the SickKids Research Institute's graduate scholarship program, Restracomp. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH). Parts of this material are based on Ontario Registrar General information on deaths, the original source of which is ServiceOntario, as well as data and information compiled and provided by the Canadian Institute for Health Information (CIHI) and Immigration, Refugees and Citizenship Canada (IRCC).
Disclaimer The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethics approval was obtained from the University of Toronto and Hospital for Sick Children Research Ethics Boards.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. The dataset from this study is held securely in coded form at ICES. While data sharing agreements prohibit ICES from making the dataset publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS. The full dataset creation plan and underlying analytic code are available from the authors on request, understanding that the computer programs may rely on coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.