Article Text

Abstract
Objectives This study is an analysis of the contribution of pre-existing medical conditions to unintentional fatal child (0–14 years) drowning and a of critique prevention stratagems, with an exploration of issues of equity in recreation.
Design This study is a total population, cross-sectional audit of all demographic, forensic and on-site situational details surrounding unintentional fatal drowning of children 0–14 years in Australia for the period of 1 July 2002 to 30 June 2012. Data were sourced from the National (Australia) Coronial Information System. Age-specific disease patterns in the general population were obtained from the Australian Institute of Health and Welfare.
Results Four hundred and sixty-eight children drowned during the study period. Fifty-three (11.3%) had a pre-existing medical condition, of whom 19 suffered from epilepsy, 13 from autism and 5 with non-specific intellectual disabilities. Epilepsy is a risk factor in childhood drowning deaths, with a prevalence of 4.1% of drowning fatalities, compared with 0.7%–1.7% among the general 0–14 years population (relative risk: 2.4–5.8). Epilepsy was deemed to be contributory in 16 of 19 cases (84.2% of epilepsy cases) with a median age of 8 years. Asthma and intellectual disabilities were under-represented in the drowning cohort.
Conclusion Except for epilepsy, this research has indicated that the risks of drowning while undertaking aquatic activities are not increased in children with pre-existing medical conditions. Children with pre-existing medical conditions can enjoy aquatic activities when appropriately supervised.
- drowning
- children
- epilepsy
- autism
- injury prevention
- water safety
- cardio-pulmonary resuscitation
- supervision
Statistics from Altmetric.com
- drowning
- children
- epilepsy
- autism
- injury prevention
- water safety
- cardio-pulmonary resuscitation
- supervision
What is already known on this topic?
Children are the age group most at risk of unintentional fatal drowning.
Medical conditions such as epilepsy are believed to increase drowning risk.
What this study adds?
Epilepsy increases the relative risk (2.4–5.8) of drowning in childhood, with a prevalence of 4.1% of drowning deaths, compared with 0.7%–1.7% among the general population.
No other identified pre-existing medical conditions were associated with an increased risk of drowning.
Heightened supervision of children around water is always warranted, including those with pre-existing medical conditions. A higher level of supervision is required for those with epilepsy.
Introduction
Drowning remains a major cause of childhood mortality worldwide,1 in both developed and developing nations.2 In Australia, children are the age group most at risk of unintentional drowning.3 Supervision that is constant, proximate and undertaken by an adult is understood to be the most effective drowning prevention strategy for children.4
Statistical and epidemiological studies that report drowning fatalities use ‘death by immersion’ as the primary designator for case finding and victim identification.2 These crude statistics mask more than 15 defined syndromes that are included under the broad term ‘drowning’.5 These disparate syndromes range from the infant who drowns in the family bathtub6 to the rescuer who drowns while attempting to rescue a child.7 It has long been known that to be effective, advocacy and interventions to reduce preventable drowning in childhood must focus on each distinct victim–site–scenario drowning syndrome.5 8 9
The question arises whether pre-existing medical conditions, such as epilepsy or physical disability, contribute to childhood drowning. In addition to the planning for effective preventative stratagems, this issue has implications relating to equality of opportunity and equity of access to aquatic activities for children with disabilities.10 Several papers have highlighted what are believed to be the increased risks of pre-existing medical conditions and drowning, particularly epilepsy.11–16 In publications sourced from many nations, including those compiled by the Royal Life Saving Society - Australia (RLSSA), there are recurring reports of children who have also suffered from pre-existing medical conditions whose deaths are included in the drowning statistics.17–20
The crucial question for future preventative and public health programmes is whether pre-existing medical conditions are primarily causal, leading to fatality, or are contributory factors conferring increased risk or are simply associative. There is a paucity of international studies concerning the contributory causal or associative specificity of pre-existing medical conditions leading to drowning. The answer to this question necessitates a total population survey, with an analysis of each individual child drowning fatality—set against the perspective of the population incidence of specific childhood medical conditions.21–24
In this paper, we report such an audit comprising a 10-year (2002–2012) national population study of every unintentional childhood drowning fatality occurring in Australia. In this study, we have linked each drowning with both a forensic review and an analysis of each child’s medical history.
Aims
The aims of this paper are to:
describe the contribution of pre-existing medical conditions leading to child (0–14 years) drowning
critique stratagems for the prevention of drowning among children with pre-existing medical conditions
explore issues of equality of aquatic recreation.
Methods
This total population study analysed the details of every child (0–14 years) who died from unintentional drowning in Australia between 1 July 2002 and 30 June 2012.
Definitions
A child was defined as an individual 0–14 years of age. This age group was chosen as drowning deaths and medical conditions in Australia are reported using 5-year age bands (eg, 0–4 years, 5–9 years and 10–14 years). Drowning has been defined using the international definition adopted by the WHO.25
Case finding
Under each state’s and territory’s legislation, drowning fatalities in Australia must be notified to the coroner by the doctor certifying death. In Australia, a nationwide coronial database is a confidential register of all deaths deemed unexpected or unnatural by the certifying doctor.26 This is a total population audit of child unintentional fatal drowning in Australia using the National (Australia) Coronial Information System (NCIS) as the primary dataset. From this, RLSSA has generated a National Fatal Drowning Database. This complete, total population database is the gold standard of unintentional drowning deaths in Australia. Cases in the database are routinely cross-referenced against the NCIS and updated as cases become closed (ie, are no longer under investigation by a coroner). Data in this study are correct as at 7 December 2016.
Exclusions
All cases of aquatic death THAT were not due to drowning (eg, shark or crocodile attack, boating injuries due to physical trauma, and so on) were excluded. Cases identified as self-inflicted harm, homicide, infanticide or the result of assaults were also excluded. Cases were included: even when no body was recovered or where only skeletal remains were found, and cases that did not have a coronial ruling at the time of analysis but where the interim cause of death was stated as drowning. At the time of analysis, 97.2% of child drowning cases used within this study were closed within the NCIS system. Perusal of the still-open cases (2.8%) suggests these are in no way atypical of the overall database.
Medical reviews
One of the authors (JP) reviewed the medical details of each case. Details of every drowning scenario, rescue, resuscitation and pre-existing medical condition were reviewed. We defined a pre-existing medical condition as one recorded in the medical history of the victim, obtained from: (A) initial police reports of the fatality; (B) from the report of the attending forensic pathologist undertaking the coronial autopsy; and (C) details from transcripts or findings of subsequent coronial inquests. For children with two or more pre-existing medical conditions (5.7%), only the leading condition was coded and used for analysis.
Causal links
For every case, two of the authors (JP and RF) together formed a collaborative interpretative judgement concerning whether the pre-existing medical condition: (A) was the direct cause of death due to drowning (eg, an epileptic seizure in the water); or (B) compromised (with fatal conclusion) any aspect of an otherwise effective rescue or successful resuscitation; or (C) was incidental to the circumstances of the drowning incident or its fatal outcome.
Data analysis and ethics
Data were recorded and reviewed for each victim’s age, sex, medical history, date of incident, date of death (if different to incident in the cases of initial non-fatal drowning), remoteness classification of drowning location, type of water hazard (eg, river, bathtub and beach), activity at time of death, visiting status, country of birth, Aboriginal and/or Torres Strait Islander status and the presence of alcohol revealed by forensic autopsy. The prevalence of relevant medical conditions in the population of Australian children 0–14 years was obtained from data published by the Australian Institute of Health and Welfare24 27–29 and The Lancet.30 Data from the US Department of Education31 was used as a proxy for Australia for the prevalence of neuromuscular disease and paralysis as no equivalent data was available for Australia. Data analysis was undertaken using IBM SPSS.32 Relative risk was calculated using the MedCalc statistical software.33
This study was approved by the Department of Justice and Regulation Human Research Ethics Committee (JHREC) (CF/07/13729; CF/10/25057, CF/13/19798).
Results
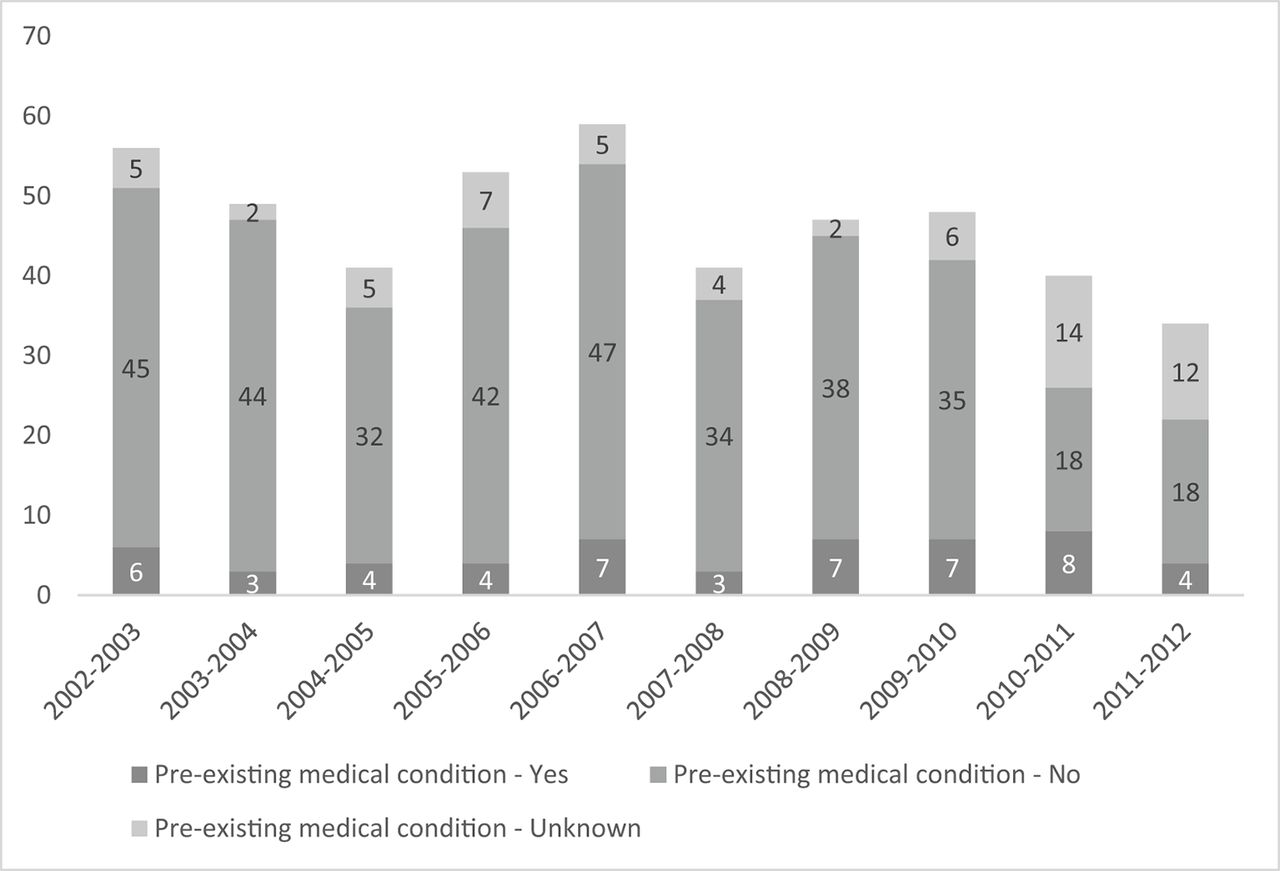
There were 2896 unintentional drowning deaths in Australia between 1 July 2002 and 30 June 2012. Of these, 468 (16.2%) were children (0–14 years) and 53 (11.3% of all fatal child drownings) had an identified pre-existing medical condition, with an average of 5.3 deaths per annum (figure 1). Males accounted for 64.7% of all childhood drowning fatalities; however, males and females were equality represented within the cohort with pre-existing medical conditions (m: 11.6%; f: 10.9%). Nineteen victims (35.8%) were aged 0–4 years, 20 (37.7%) were aged 5–9 years and 14 (26.4%) were aged 10–14 years (table 1).
{kind=link}
Child (0-14 years) drowning deaths and status of pre-existing medical conditions, by financial year. Total population survey, Australia, 2002/03–2011/12 (N=468).
Patterns of pre-existing medical conditions, by age and sex. Total population survey of all child drowning deaths, Australia, 2002/03–2011/12 (N=468)
Fifty-three children suffered from a pre-existing medical condition (table 2). Children with pre-existing medical conditions were on average older (7.0 years) than those children without pre-existing medical conditions (3.7 years). Children with pre-existing medical conditions drown in similar circumstances to those without. Children with pre-existing medical conditions commonly drowned in swimming pools (32.1%), bathtubs and rivers (18.9% respectively), as a result of falls into water (49.1%) and while swimming (22.6%) and bathing (20.8%). Location of drowning and activity prior to drowning were not found to be statistically significant for children with pre-existing medical conditions.
Drowning deaths of children with pre-existing medical conditions, by diagnosis, age, sex and incidence. Total population survey, Australia, 2002/03–2011/12 (n=53)
Alcohol was found to be present in 3.8%, though it was not found to be statistically significant. Four victims were known to be Aboriginal and/or Torres Strait Islander. Almost half (43.4%) of drowning deaths occurred in areas classified as major cities, with a further 7.5% taking place in remote and very remote locations. The majority of victims (86.8%) were not visitors.
Children with epilepsy (35.8%) included those with primary diagnoses of a seizure disorder, Landau Kleffner Syndrome, persistent febrile convulsions and Lennon-Gastaut syndrome. Other medical conditions (11.4%) included diagnoses such as Down syndrome, cystic fibrosis, fetal alcohol syndrome and Duchenne muscular dystrophy. Epilepsy is an associated risk factor in childhood drowning deaths, with a prevalence of 4.1%, compared with a prevalence of 0.7%–1.7% among the general 0–14 years age population (RR: 2.4–5.8 (95% CI 1.3 to 13.7)). The median age of children who drowned with a diagnosis of pre-existing epilepsy was 8 years (range 2–14 years).
Intellectual disabilities (RR: 0.2; 95% CI 0.1 to 0.6) and asthma (RR: 0.05–0.09; 95% CI 0.0 to 0.3) were associated with a lower risk of drowning than that in the general population.
The analysis and interpretation of the links between pre-existing medical conditions and fatal drowning are shown in table 3. In 16 children (30.2% of the 53 children with an identified pre-existing medical condition), their pre-existing medical condition had no impact on the drowning event. For example, the fact that a toddler had cystic fibrosis was incidental to his wandering away from a family picnic and drowning in an ornamental pond nearby (table 3).
Attributed pre-existing medical conditions. Total population survey, Australia, 2002/03–2011/12 (n=53)
One child had Down syndrome, and another was developmentally delayed (and suffered epilepsy), which we deemed contributory to the drowning. We deemed several pre-existing conditions other than epilepsy (eg, autism, intellectual disability, neuromuscular disease and myocarditis) possibly or directly contributory to the drowning in 20 cases. No child with cerebral palsy, uncomplicated by epilepsy or other condition drowned.
Among the 16 victims where epilepsy was deemed to be a direct cause: 14 were born in Australia (the country of birth was unrecorded in two cases). Two children were identified as of Aboriginal and/or Torres Strait Islander descent. None were overseas visitors. Two-fifths (43.8%) were aged 10–14 years, with only one victim under 5 years of age. Five children were in a bathtub and bathing at the time (aged 3–14 years), five were in swimming pools, two were at the beach, two were in rivers, one was in a lake and one in a dam (table 4). None were appropriately supervised at the time.
Location grouping by activity grouping for children with direct cause epilepsy, child (0–14 years) drowning deaths. Total population survey, Australia, 2002/03–2011/12 (n=16)
Discussion
In this study, 11% of all childhood unintentional drowning victims had an identified pre-existing medical condition; this was lower than that which was found by Schyllander et al (16%).34 Similar to other studies, two-thirds (65%) of childhood drowning fatalities were male34 35; however, males and females are equally represented within the cohort with pre-existing conditions. Children with epilepsy commonly drowned in aquatic environments in and around the home, such as bathtubs (31%) and swimming pools (31%), and none were adequately supervised at the time of their drowning.
At the outset of this research, we posited that pre-existing medical conditions increase the risk of fatal drowning by one or more of three mechanisms: (A) the pre-existing condition (eg, autism)36 might increase the likelihood of a child inappropriately seeking and entering a water hazard; (B) the condition might increase the risk of drowning once the potential victim is in the water (eg, frailty or muscular paresis or paralysis); or (C) reduced rates of successful resuscitation or successful intensive care outcomes due to pre-existing medical conditions (eg, cystic fibrosis).
In the context of current supervisory practices that relate to children with pre-existing medical conditions, this study has confirmed that there is no increased risk for children with delayed social and intellectual development. Rather, intellectual disabilities and asthma were associated with a lower risk of drowning than that in the general population. We posit that this association is related to decreased exposure to aquatic hazards and to instinctive heightened supervision of children.10 This applies particularly to frailty, due to sarcopenia particularly of neuromuscular diseases. We believe that this is one reason why this research has not revealed an increased risk to such children, apart from those with epilepsy. An assessment of the mathematical increase in risk necessitates the compilation of exposure denominators that are unknown and probably unknowable for this group of conditions. Children with a priori medical condition may not have had an equal opportunity for swimming lessons30 and as such might be at greater risk of drowning. The only pre-existing condition that leads to an increased risk of fatal drowning, under current real-life conditions of supervision, once a child is in the water, is epilepsy. Again, there is a relative increase but the absolute mathematical risk remains small and maybe zero with compensatory supervision.5 We posit that multiple, pre-existing medical conditions, specifically associated with epilepsy, may contribute to the risk of drowning, further work is required to elucidate this point.
In the aquatic domain, there are obvious extra demands in the care and supervision of an individual child with a history of epilepsy, or in other conditions such as those with a family history of the long QT (QTc) syndrome.37 No appropriately supervised child drowned in Australia over the 12-year survey period. Supervision is a complex skill requiring the four elements of proximity, continuity, attention and preparedness for it to be effective.8 Children with epilepsy may swim with safety if (A) anti-convulsant drug blood concentrations are in the therapeutic range; (B) the child has been seizure free for 6–12 months; and (C) compensatory extra supervision is in place.5
Advocacy for, and the implementation of, safety barriers (ie, barriers that prevent access) around water hazards (especially domestic pools and ponds), have dramatically reduced the rates of childhood drowning.8 9 38 Such safety barriers are particularly important in the prevention of drowning if children have pre-existing medical conditions especially frailty from any cause and those with intellectual disability.
If rescuers are trained in cardiopulmonary resuscitation, there is a 30%–40% chance of turning a potential fatality into a survivor.11 39 Every parent should have a current first aid certificate, a policy of significance for parents of children with disabilities. Swimming skills are important life skills; and children with chronic medical conditions and congenital disabilities need these no less than able bodied children.10 Common sense indicates that swimming lessons should be conducted as a one-on-one format and appropriate strategies implemented to ensure the child’s safety in the water.10 Life jackets, for children at increased risk of a seizure, that will roll them onto their back and keep their nose and mouth out of the water during a seizure may prevent drowning.40
This study is the first longitudinal total population analysis of the prevalence and role of pre-existing medical conditions in unintentional fatal drowning among children aged 0–14 years using unselected, total population coronial data. The use of coronial data allows for a deeper understanding of the presence of pre-existing medical conditions as identified by forensic pathologists by accessing coronial autopsy reports. There were a small number (13.2% of all unintentional child fatal drownings) of cases where pre-existing medical condition was unknown. This was due to no information being available about the status of the pre-existing medical condition due to the autopsy document not being available, no mention being made of pre-existing medical conditions in the case documentation or that the parents did not want an autopsy to be undertaken. There were also six cases associated with a mass flooding and casualty event in the 2011/12 financial year where autopsies were not undertaken.
This study examined fatal drownings only; it should be noted that it is not known if the non-epilepsy chronic medical condition related non-fatal drownings have higher rates of severe morbidity. Studies of this nature of necessity depend on the subjective assignment of causal roles leading to injury. We believe that the expertise of the two experienced reviewers (paediatrician and neurologist, and safety analysis expert) provide current best subjective review of such causality.
Conclusion
There are nuances in the relationship between pre-existing chronic illness and the risk of childhood drowning. This study shows that the mathematical risks of aquatic activities are not dangerously increased in children with pre-existing medical conditions, when compared with the baseline population. Awareness of prevention strategies and the need to ensure heightened vigilance of children with pre-existing medical conditions, particularly those with epilepsy, is required. Children with pre-existing medical conditions should not be denied the joys and developmental experience of aquatic activities.
Acknowledgments
This research is supported by the Royal Life Saving Society - Australia to aid in the reduction of drowning. Research at the Royal Life Saving Society - Australia is supported by the Australian Government.
References
Footnotes
Contributors RCF and JHP conceived the study. AEP sourced the data. JHP and RCF reviewed the medical details of each case. JHP and RCF formulated an interpretive judgement concerning whether the pre-existing medical condition was a direct cause, compromised a fatal drowning or was incidental. RCF conducted the analysis and wrote the manuscript. JHP assisted in the analysis and reviewed the manuscript. AEP reviewed the manuscript.
Disclaimer The lead author, RCF, affirms that the manuscript is an honest, accurate and transparent account of the study being reported, that no important aspects of the study have been omitted and that any discrepancies from the study as planned (and if relevant, registered) have been explained.
Competing interests None declared.
Patient consent Victims are deceased and data is stored by the data custodians, the Australian National Coronial Information System (NCIS). Access to researchers is governed under strict ethical protocols.
Ethics approval Department of Justice Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement With respect to the data set underlying this research, these data are available on request. However, as the data have been accessed via a third party (coronial data), ethical approval and permission from the data custodians, the Australian National Coronial Information System (NCIS) is required before the authors are able to provide their data set to the person inquiring. There are strict ethical restrictions around the use of these data, and it can therefore not be sent to a public repository. Once ethical approval and permission from the NCIS as data custodians has been achieved, researchers can contact richard.franklin@jcu.edu.au to gain access to the data.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with ’BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected these errors and the correct publishers have been inserted into the references.