Article Text

Abstract
Increasing numbers, complexities and technology dependencies of children and young people with life-limiting conditions require paediatricians to be well prepared to meet their changing needs. Paediatric Advance Care Planning provides a framework for paediatricians, families and their multidisciplinary teams to consider, reflect and record the outcome of their conversations about what might happen in the future in order to optimise quality of clinical care and inform decision-making. For some children and young people this will include discussions about the possibility of death in childhood. This may be unexpected and sudden, in the context of an otherwise active management plan or may be expected and necessitate discussions about the process of dying and attention to symptoms. Decision-making about appropriate levels of intervention must take place within a legal and ethical framework, recognising that the UK Equality Act (2010) protects the rights of disabled children and young people and infants and children of all ages to the same high quality healthcare as anyone else.
- Children's Rights
- Ethics
- Neurodisability
- Palliative Care
- Paediatric Practice
Statistics from Altmetric.com
Introduction
This article sets out to:
-
Describe paediatric Advance Care Planning (pACP) and its various elements;
-
Discuss the evidence to support pACP;
-
Give pragmatic guidance about pACP for paediatricians based on extensive personal experience;
-
Discuss the tricky areas of prognostication and decision-making about appropriate levels of intervention that underpin pACP.
What is paediatric Advance Care Planning and why do it?
Advance Care Planning (ACP) has different meanings depending on perspective of country and legislation.1 In broad terms it is a description of the process of discussing issues and planning ahead in anticipation of a change in condition in future. The components of pACP for some families will include discussions about the possibility of premature death. If these conversations are not had, families will miss out on opportunities to state their wishes for aspects of care and interventions, including place of care and preferred place of death.2 Clinician-led discussions about the possibilities of dying and death in advance may help families to communicate among themselves about what may otherwise have remained unspoken, may help with the grieving process and improve realistic hope and resilience.3
What is the evidence to support Advance Care Planning in paediatric clinical practice?
The prevalence of life-limiting conditions in children is increasing,4 bringing an increasing clinical need to recognise when dying and death may be possibilities, so that appropriate discussions can be had with families. Balanced against a dearth of randomised, controlled trials in the area of pACP,5 ,6 decision-making about appropriate levels of intervention and end-of-life care for children,i there are plenty of qualitative and descriptive publications evidencing good clinical practice. The Royal College of Paediatrics and Child Health is currently updating their guidance on decision-making for children with life-limiting conditions and the National Institute for Health and Care Excellence (NICE) in England is planning a clinical guideline on end-of-life care in children, both eagerly anticipated; it will be interesting to see how much evidence their rigorous processes identify.
One key message from the literature is without doubt: planning and care for children at risk of premature death needs to improve. A systematic review (2013) reported on three pACP programmes in the USA, two developed from adult programmes.1 These involved discussions with families in advance, involvement of chaplains and recording of ‘advance directives’. Preliminary findings were that pACP can be implemented and was perceived as helpful. A randomised controlled trial specific to HIV-infected adolescents5 showed pACP to trigger positive emotional experiences in young people and their carers with less negative reactions when compared with those in the study's control arm not receiving pACP, also a better communication experience and marginally improved certainty about decisions in the intervention group.5 ,7 A subsequent randomised controlled trial of family centered pACP in young people with cancer concluded that those receiving pACP were significantly better informed about end-of-life decisions and the young people were more likely to allow family members to ‘do what is best at the time’ (100%) compared with the control group who did not receive pACP (62%).6 Those in the pACP group were significantly more likely to limit treatments, knowing that this accorded with the young person's own wishes.
Consistently across studies young people and their carers wanted more information and to be involved in decision-making.7–12 Reported barriers to pACP included lack of many children's capacity to be involved in decision-making themselves, the high degree of prognostic uncertainty, unrealistic expectations of parents, doctors’ worries about removing hope and complexity of the social environment.13–15 In one study 71% of doctors questioned thought pACP happened too late.15 No studies compared frequency of home deaths in children with and without pACP, but two studies suggest home deaths may be more frequent where pACP had occurred.16 ,17
A study on Birmingham's paediatric intensive care unit captured views of eight consultants and six senior nurses.18 They felt that children were ‘enduring’ intensive care which they believed to be ‘futile’ and expressed the view that pACP was lacking, but if implemented would improve care for children with life-limiting conditions.
Elements of paediatric Advance Care Planning
Emergency healthcare planning
It is good clinical practice to provide for families with children with complex healthcare needs a written care plan that includes information about their diagnoses, active health concerns and any emergency scenarios that can be predicted to arise, including written guidance about what to do from presentation in the community through to the hospital emergency department (see figure 1). This is promoted in the UK through ‘Together for Short Lives’ (http://www.togetherforshortlives.org.uk) who have many helpful supporting resources for families and professionals. A national survey of UK paediatric intensive care units found wide variation in availability and nature of formal pACP documents and called for development of national policy informed by review and evaluation of existing documents and current practice in pACP.19

Component elements of paediatric Advance Care Planning.
In 2011, the Department of Health (England) funded a collaboration of paediatricians representing general, community, emergency, disability and palliative care paediatrics who together with the Council for Disabled Children agreed core principles for Emergency Health Care Plans. It was acknowledged that localities required their own easily recognisable formats for such Plans across services, including Ambulance Services. The outputs from this work, including e-Learning resources, regional exemplar templates, a parent information leaflet and video exemplars of enacted difficult conversations with families can be found at: http://www.councilfordisabledchildren.org.uk/ehp.
Advance statement of wishes and preferences
Fraser and team from Bristol have led on this work in the UK.20 Practical templates, flow charts and resources are accessible at http://www.togetherforshortlives.org.uk/professionals/external_resources/
Statement about discussions with the child and parents about appropriate levels of intervention and the circumstances in which these will apply
This is the trickiest area, as there is a need for the paediatrician to have discussed the issue of prognosis with the child, their parents or guardians. Prognostication can be extremely difficult; it falls into two broad groups:
-
Risk of sudden and unexpected premature death in childhood
-
There is evidence that children with long-term conditions are at higher risk than others of sudden and unexpected death.4 Paediatricians are not universally confident about discussing this risk with families9 ,15 ,18 ,19 but increasingly need to see this as part of their role.
-
Paediatricians may be familiar with the concept of Sudden Unexpected Death in Epilepsy. Recent evidence suggests that it is the complexity of the child's disabilities rather than the epilepsy itself that is the main risk factor for sudden death.21 There is also evidence especially from support groups (eg, http://www.epilepsyaction.org.uk ; http://www.sudep.org) that families deal better with their loss and grief if there had been a discussion about risk of death in advance. Thus paediatricians caring for children with long-term conditions, especially those with complex disabilities, need to consider the possibility of death and discuss risks openly with families. Discussing the possibility of death does not mean that active treatment should cease. It should never be assumed that early death is inevitable and pACP always needs to embrace a range of possible outcomes.
-
Clinicians should be mindful of the improved survival opportunities for even those with complex disabilities, who may not follow the journey predicted for their condition in the published literature and who may respond well to intensive care to tide them over episodes of acute illness. The multifaceted needs of the child should continue to be addressed, based on best evidence, aiming always for the best possible quality of life and fullest possible participation in everyday activities.22
-
The mode of death in the sudden, unexpected group is as it says on the tin and can occur at any time, in any setting, most usually at night. Families need to be sensitively made aware of this, while setting the risk in context and not making them overanxious.
-
-
Risk of gradual decline, dying and death
-
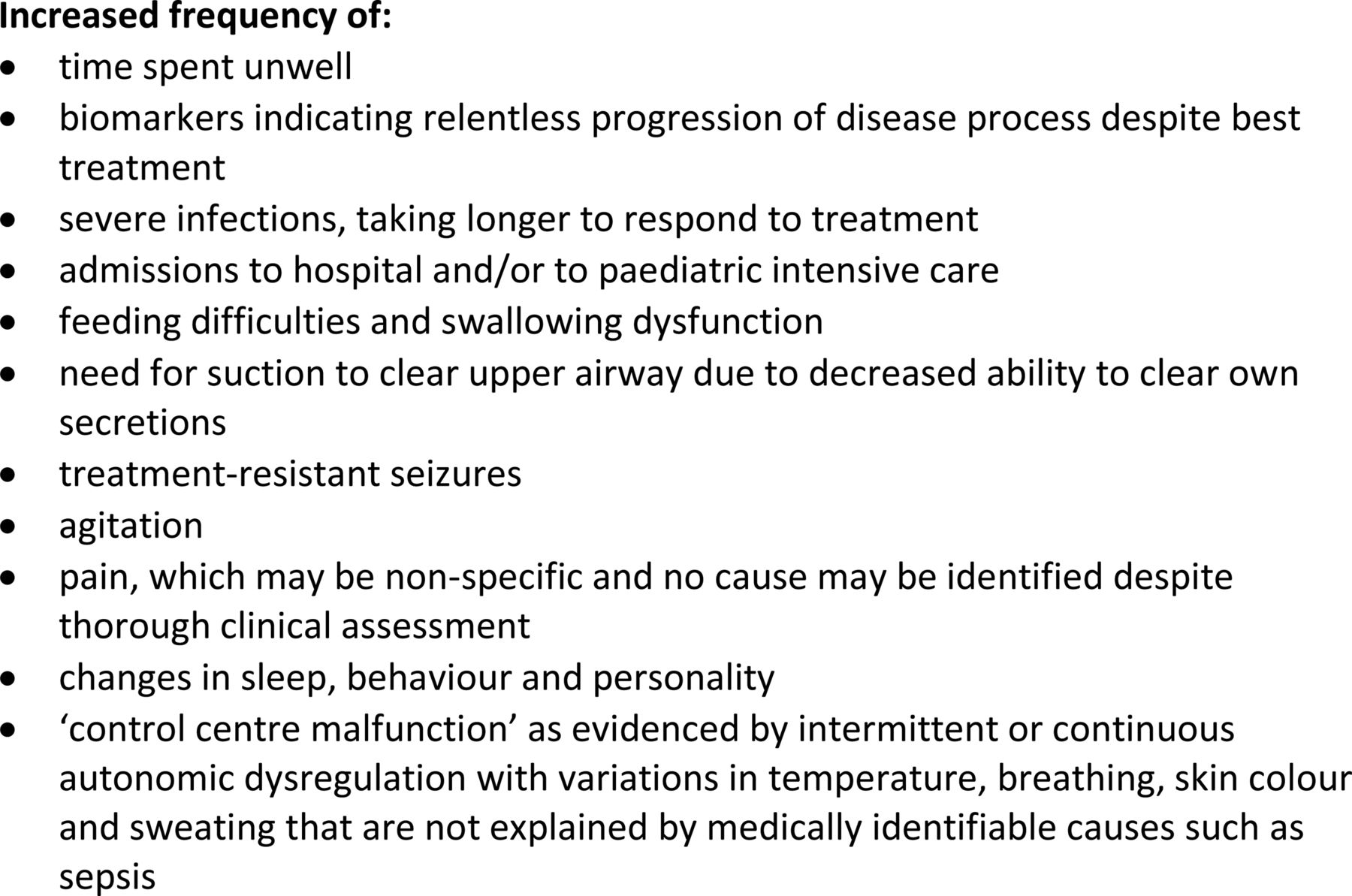
Identifying this group requires the paediatrician to be alert for ‘red flags’ that the dying process may be imminent or occurring. Some suggested ‘red flags’ from personal experience are listed in figure 2.
-
Children at risk include those:
-
for whom active treatment is no longer effective and/or the disease process is progressing;
-
with an underlying static medical condition, usually neurological, chromosomal or genetic, where secondary complications develop their own momentum, unchecked by best efforts of medical interventions.
-
-
The conversation with families about risks of dying and death for this group is necessarily different, as the clinician is sensitively letting the family know that death is expected, although the precise timing of death cannot be predicted and even the frailest children continue to surprise us with their remarkable resilience.
-
It should be acknowledged by the clinician that resuscitation attempts are likely to be unsuccessful and that further active treatments are likely to be futile; both may be burdensome for the child and distressing for the family. This needs to be recorded on the family held care plan so that the lead clinician at all times is appraised of what has been discussed and with whom.
-
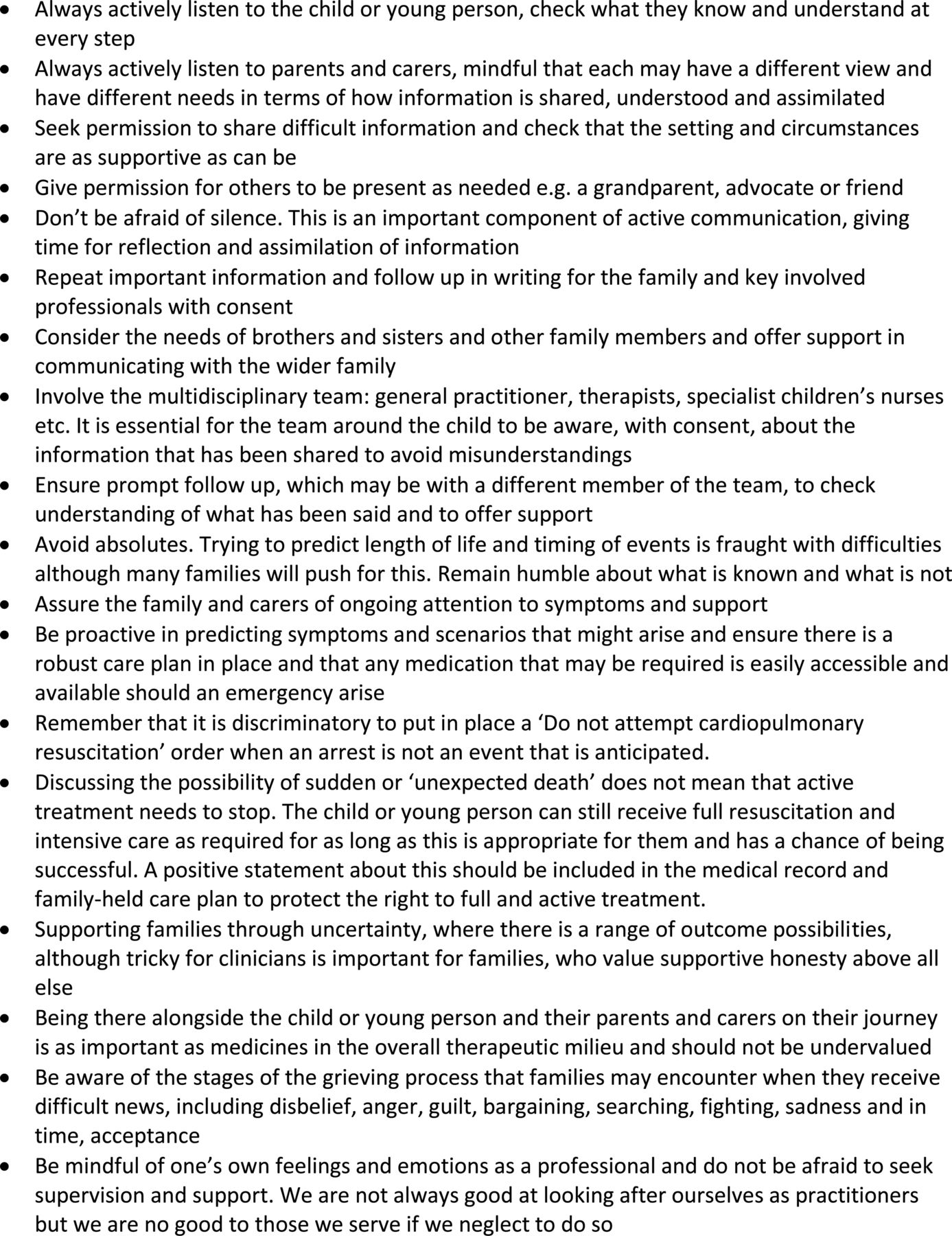
Having a conversation with a family about the possibilities of dying and death is difficult for all involved and requires careful thought and preparation. Some tips from personal experience to consider are given in figure 3.
-
If death is inevitable in the clinical judgment of the lead clinician and a decision is made that further life-sustaining treatment is inappropriate and would be burdensome, there are a number issues to take into account, including in any pACP documentation (see figure 4).
-
The mode of death for this group is more likely to be gradual, most often with significant respiratory failure compounded by atelectasis and variable infection all of which may contribute to symptoms that will need to be addressed to ensure comfort at all times and explained to the family. Families may get upset about the length of time that the dying process can take. Being alongside them at this difficult stage of their child's journey and continuing to offer explanation and support is an important role of the clinical team and much appreciated by families.
-

Red flags that dying and death are significant possibilities in children and young people who are medically frail.
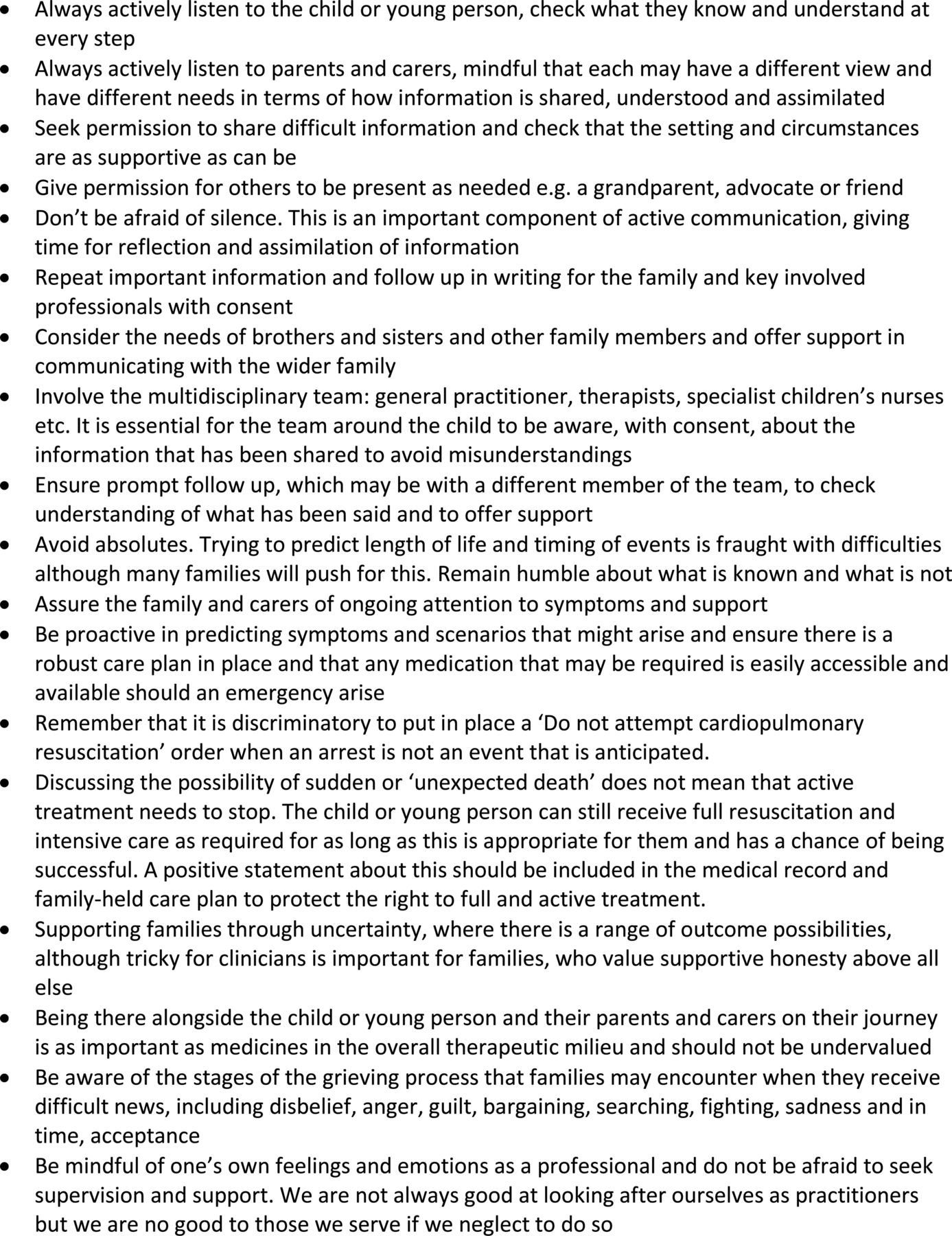
Tips to consider when planning a conversation about the possibilities of dying and death of a child or young person.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Checklist if dying and death may be possible.
Decision-making frameworks
All decision-making must be within an ethical and legal framework. In the UK clinicians are bound to follow the 2010 General Medical Council guidance on treatment and care towards the end of life that includes specific guidance on decision-making for children and young people23 and also the Equality Act (2010)24 that includes disability and age among the protected characteristics that must not be used as a reason to treat some people worse than others. The Children Act (1989 and 2004) applies throughout the UK and includes a seven-point welfare checklist that must underpin any decisions made in the courts or best interests decisions about children and young people up to 18 years of age.25 In England and Wales those aged 16 years or more come under the 2005 Mental Capacity Act (MCA) that defines tests of capacity and sets out a minimum nine-point checklist for estimating the best interests of a person who lacks capacity.26
The process of decision-making as well as the actual decision should be written in the medical record and also in any family held care plan, so that in the event of a healthcare emergency it is clear to all who may be involved as to what has been discussed and decided, in the child's best interests.
Advance Care Planning with and for children under 16 years of age
In UK law, children under 16 years of age are presumed to be incompetent to make their own decisions, although legal mechanisms exist that allow them to demonstrate their competence for specific decisions, for example, Fraser guidelines and Gillick competence test.27 While legally competent to make some decisions about themselves, young people face the extra challenges of adolescence including emerging and variable maturity and concrete thinking. The paediatrician, mindful of these complexities, should refer to the Children Act (1989 and 2004) welfare checklist25 to guide any decision made by, with or on behalf of children and young people in their best interests.
Advance Care Planning with and for 16-year-olds and 17-year-olds and transition issues
There is a presumption in law in England and Wales that 16–17-year-olds have capacity to consent to treatment and can refuse some treatments. For those assessed to lack capacity, a person with parental responsibility, usually a parent, should be consulted by the clinician who will make a decision in the young person's best interests. Also, the Children Act (1989 and 2004) allows a parent to consent to treatment as for a younger child. It may be necessary to seek legal advice in case of uncertainty or disagreement.
In Scotland, 16-year-olds are considered to have capacity and can consent or withhold consent for themselves in the same way as a person 18 years of age or over in England and Wales under the MCA. For a young person in Scotland assessed to lack capacity for specific decisions, a power of attorney may be appointed by application to the Office of the Public Guardian (Scotland).28
In North-East England, a collaboration of palliative care physicians and paediatricians produced an all-age suite of support tools for decision-making and recording that is also being adopted in other regions.29 This overcomes difficulties that otherwise might arise at transition between children's and adult services, where ‘best interests’ may be differently defined.
Whatever process is adopted, it is essential to be mindful of the MCA best interests process for all young people over 16 years of age who lack capacity for a specific decision at a specific time and in specific circumstances.
Conclusions
In the face of increasing numbers of children with life-limiting conditions, paediatricians need to be well prepared to plan ahead for clinical scenarios that might arise, to recognise when unexpected or expected death may be possible and to discuss risks openly with families. This allows the child where possible and their parents and carers, to express and record their wishes and preferences and for conversations to be had between the family and multidisciplinary team about appropriate levels of interventions. Increasing the number of conversations about dying and death with families and improving recording of wishes and decision-making using a pACP framework will facilitate future research to explore pACP more thoroughly, with the hope of making the most difficult journey of all for families a little more bearable.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.
-
↵i ‘Children’ is used throughout the article as synonymous with ‘children and young people’